

Your surgeon drained you, sutured you, wrapped you in a faja, and sent you home. Most patients are also sent with abdominal boards or lipo foam to wear inside the garment. Within 24 to 48 hours, the swelling begins. Not the gradual kind you expected. The tight, hot, board-hard kind that convinces patients something catastrophic has happened. What is actually happening is predictable, well-documented physiology, and lymphatic drainage massage is the single most evidence-supported tool to move it through faster. But the timing matters. Starting too late forfeits the critical early window. Starting too aggressively before the drainage slows can displace fluid into unintended tissue planes. This protocol tells you exactly when and how. The schedule below tracks the guidance ASPS member surgeons publish: board-certified plastic surgeon Dr. Christian Subbio notes that lymphatic massage helps prevent fibrosis and contour irregularities and facilitates lymphatic drainage for a smoother, more even result, and many ASPS surgeons have patients begin the day after surgery and continue several times a week for about two months.
The short answer
Lymphatic massage typically begins 24–72 hours after surgery, starts at 3–5 sessions per week in the first month, and tapers to 1–2 sessions per week by week six to eight. Your surgeon’s specific instructions take priority over any general schedule.
Why Your Lymphatic System Needs Help After Liposuction
Liposuction is a mechanical disruption. The cannula physically severs lymphatic capillaries, the paper-thin vessels responsible for draining interstitial fluid back into circulation. In a healthy, undisturbed tissue bed, these capillaries passively absorb excess fluid and return it to the bloodstream via lymph nodes. After lipo, that network is temporarily offline in the operative zone. Fluid accumulates. The body deploys inflammatory mediators to begin repair. The result is pronounced edema, localized pressure, and the characteristic hardness that peaks around weeks two to four.
Manual lymphatic drainage (MLD) accelerates the process your body is already trying to complete. By applying specific, rhythmic, low-pressure strokes, a trained therapist stimulates the intact lymphatic vessels at the periphery of the surgical area to increase their contractile frequency. This creates a suction effect that draws stagnant fluid away from the congested zone and routes it toward functioning lymph nodes in the groin, axilla, or thorax. Clinical data from the Journal of Plastic and Reconstructive Surgery consistently shows that patients who begin MLD within the first 72 hours of surgery demonstrate measurably faster resolution of edema compared to controls.
The secondary benefit addresses fibrosis prevention. When inflammatory fluid sits undrained in tissue for extended periods, fibroblasts deposit collagen in a disorganized pattern. This is the mechanism behind post-lipo fibrosis, the hard, rope-like nodules and irregular texture that form beneath the skin. Lymphatic massage, by keeping fluid mobile, reduces the substrate for fibrotic adhesion formation. If you have already noticed firm, irregular patches beneath your skin, read the full clinical breakdown in our article on how to manage hard lumps and fibrosis after liposuction.
| Phase | Sessions | Notes |
|---|---|---|
| Day 1–3 | 0–1 sessions | Only if surgeon clears immediately post-op |
| Day 4–7 | 3–5 sessions | Gentle only, trained therapist recommended |
| Week 2–4 | 3–5 sessions per week | Focus on areas of firmness and fluid |
| Week 4–6 | 2–3 sessions per week | Taper as swelling reduces |
| Week 6–8 | 1–2 sessions per week | Maintenance phase |
| Week 8+ | As needed | Target remaining fibrosis or firmness |
What a Standard Post-Op Session Looks Like
The first session, typically performed 24 to 48 hours post-operatively either by a clinic nurse or a certified MLD therapist, is not a deep tissue massage. Patients who confuse the two often report bruising their fresh surgical sites or triggering seromas. A standard immediate post-op session follows this structure.
Opening the pathways (5 to 8 minutes): The therapist begins far from the surgical site, working the cervical lymph nodes at the neck and the axillary nodes in the armpits. This “empties” the downstream vessels so they have capacity to receive the fluid that will be moved toward them.
Working the periphery inward (15 to 20 minutes): Light, J-stroke and circle-pump techniques move outward from the surgical borders. The pressure applied is deliberately gentle, equivalent to the weight of a coin on the skin. Anything deeper compresses the capillaries closed rather than stimulating them open.
Feathering the primary zone (10 minutes): Only after peripheral pathways are primed does the therapist address the operative tissue directly. Strokes travel in the direction of the nearest lymph node basin, never randomly or in circular patterns across the surgical field.
Closing sequence (5 minutes): The session ends with return strokes to the cleared nodes, helping the routed fluid complete its transit. The patient is then re-dressed in their compression garment, which maintains mild external pressure to prevent fluid from re-pooling — see the guide on when to switch between your Stage 1 and Stage 2 faja for guidance on what garment to pair with each phase.
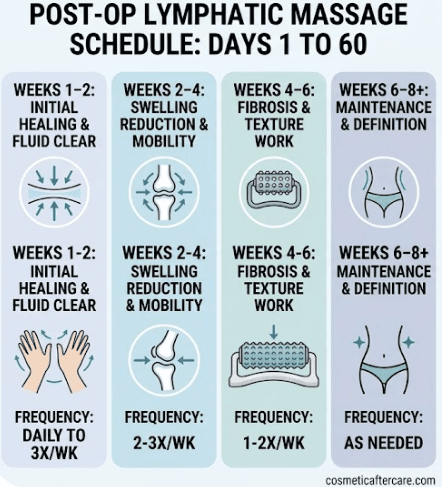
The Four Phases of Massage Frequency: Days 1 to 60
Massage frequency is not static. Your tissue is at a completely different biological stage at week one than it is at week six, and the protocol should reflect that. Below are the four distinct clinical phases that govern post-lipo massage scheduling.
MLD is also used for chin liposuction, typically starting in week 2 once acute swelling has settled. The submental area responds well to lymphatic drainage. More on the full chin liposuction recovery timeline, including when MLD is appropriate.
Phase 1: Weeks 1 to 2, Initial Healing and Fluid Clearance
This is the highest-volume phase. Fluid production is at its peak, drainage channels are disrupted, and the inflammatory process is most active. The clinical goal is pure volume reduction: get the fluid moving before it stagnates. The recommended frequency is daily sessions if possible, with a minimum of three sessions per week. Sessions at this stage focus on gentle suction-stimulation techniques and should never apply pressure directly over the drainage sites if drains are still present. If your surgeon placed a drain, leave the tissue around it undisturbed.
Phase 2: Weeks 2 to 4, Swelling Reduction and Mobility
Acute edema begins to subside, but the tissue is still actively remodeling. Lymphatic channels are partially regenerating. You may notice the swelling fluctuates: better in the morning, worse in the evening — many patients are alarmed by this, and if that’s you, why you look bigger after lipo explains what’s happening. This is normal and reflects the body’s inability to fully drain by gravity alone after a day upright. During this phase, two to three sessions per week remains the clinical standard. The therapist can now begin introducing slightly deeper techniques in areas where the superficial edema has cleared, targeting the thicker, more structured fluid collections that persist deeper in the tissue.
Phase 3: Weeks 4 to 6, Fibrosis and Texture Work
The composition of the problem shifts. You are no longer primarily fighting fluid. You are fighting the early deposition of collagen in disorganized patterns beneath the skin. This is the fibrosis formation window, and massage must adapt accordingly. Techniques become more focused, using sustained pressure and specific myofascial release strokes to break up forming adhesions. Frequency drops to one to two sessions per week because the goal is mechanical mobilization of firming tissue rather than fluid transport. This is also the phase where patients who skipped earlier sessions often begin noticing concerning texture changes.
Phase 4: Weeks 6 to 8 and Beyond, Maintenance and Definition
By week six, most patients have cleared 70 to 80 percent of their initial swelling. The remaining puffiness is residual and will continue to resolve over months as the body completes its internal remodeling process. Massage in this phase is maintenance-focused: preventing recurrence of adhesion formation, supporting skin retraction, and ensuring the tissue settles smoothly. Sessions are as-needed, typically once every one to two weeks. Some patients extend this phase through month three or four if they notice persistent firmness in specific zones.
Professional Massage vs. DIY: What Is and Is Not Safe at Home
The rise of at-home lymphatic massage tutorials on social media has created a significant problem in post-op recovery communities. The techniques look simple: gentle, rhythmic strokes in a clear direction. What the videos cannot convey is the depth of training required to correctly identify the direction of lymphatic flow in an altered tissue landscape, assess which nodes are actively draining versus congested, and adjust pressure in real time based on tissue response. Getting this wrong does not just mean the massage is ineffective. It can mean redirecting fluid into an area where it cannot drain, creating or worsening a seroma, or applying mechanical force over a compromised suture line.
For the first four weeks post-operatively, professional MLD from a therapist certified specifically in post-surgical lymphatic drainage is the standard of care. Look for Vodder or Casley-Smith method certification, both of which include post-surgical protocols in their training curriculum.
What you can safely do at home after week four, once your surgeon has cleared you, is light self-drainage between sessions. Keep the following rules clear. Use only fingertip pressure, never your palm. Always stroke toward the nearest clear lymph node basin, groin for abdominal lipo, armpit for flank lipo. Never massage directly over an incision, drain site, or any area your surgeon has designated as restricted. Do not use massage oils, lotions, or vibrating tools unless specifically cleared by your surgeon. Limit self-drainage to ten minutes per session. If you feel increased swelling, pain, or warmth after self-drainage, stop immediately and contact your surgical team.
Recommended: Fibrosis Roller
Between professional lymphatic sessions, a firm handheld roller keeps gentle, consistent pressure on developing hard spots at home, and this fibrosis roller is the low-cost version of the tool many post-op massage therapists use in session.
Wood therapy tools and cupping, commonly promoted in recovery communities, are contraindicated during the first six weeks post-lipo. These apply suction or compressive forces at a depth that can disrupt organizing tissue and increase fibrosis risk rather than reduce it. If a therapist recommends these tools before your six-week mark, seek a second opinion.
This is normal
- Temporary increase in swelling for 24 hours after a session
- Mild bruising at massage sites in early weeks
- Feeling of fluid movement during the massage
Call your provider if
- Fever following a massage session
- Sudden significant increase in swelling after week four
- Open skin or wound at any massage site
The protocol above applies equally to VASER liposuction patients. Because VASER generates thermal energy that disrupts lymphatic channels more significantly than standard liposuction, early and consistent lymphatic massage is, if anything, more important after VASER than after standard lipo. The VASER liposuction recovery guide covers how the seroma risk and other aspects of VASER recovery differ from what this schedule describes.
This article is for educational purposes only and is not a substitute for professional medical advice. Always follow your injector’s or surgeon’s specific aftercare instructions.