

You lost the weight. Maybe forty pounds, maybe sixty. The GLP-1 medication did exactly what it was supposed to do, and you look in the mirror and notice something unexpected: your face looks older, hollower, like the skin forgot to follow the fat out the door. Nobody mentioned this part at the consultation.
“Ozempic face” is what the internet started calling it, as if the drug were doing something sinister to your facial tissue. It is not. What you are seeing is a fat redistribution problem that has nothing to do with the specific medication and everything to do with how fast you lost the weight. The same pattern plays out with newer triple-agonist compounds like retatrutide: faster weight loss means more pronounced facial changes, regardless of which drug caused it. The same mechanism is behind the same thing happening below the neck, in the breasts and buttocks, for the exact same reason.
What Is Actually Happening Under Your Skin
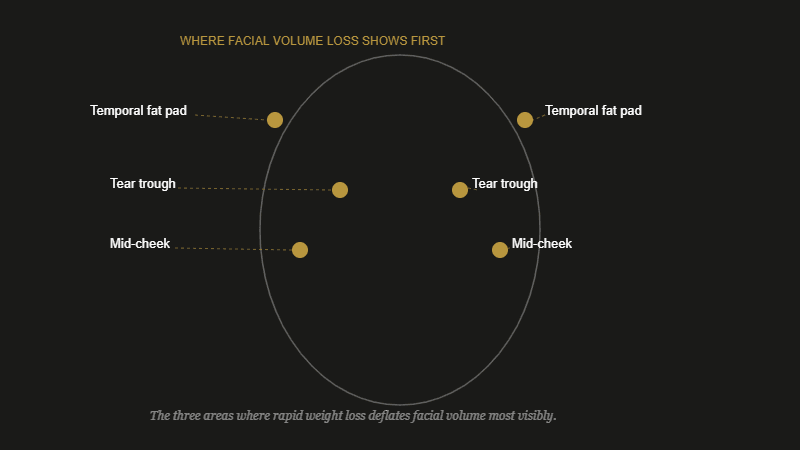
Your face has a network of discrete fat compartments, called facial fat pads, layered at different depths. The ones in your temples, mid-cheek, and under your eyes are responsible for the soft, lifted, three-dimensional quality that reads as youthful. They are not the same fat as what sits on your belly or hips. But they are still fat, and when you lose weight rapidly, your body draws from all its reserves, including these facial compartments.
The face tends to show weight loss disproportionately. It has less fat to lose than the trunk, so proportional losses are more visually dramatic. Lose ten percent of your body weight and your abdomen might look slightly slimmer. Your cheeks might look noticeably deflated.
Rate matters more than total amount. A slower loss gives the overlying skin more time to adapt. A faster one leaves the skin and the connective tissue structure that used to be supported by volume with nothing to hold against. The result is the hollowing and sagging at the temples, the deepened nasolabial folds, the newly visible tear trough at the inner corner of the eye socket.
Why the Under-Eye Area Looks Worst
The tear trough is the groove that runs from the inner corner of your eye toward the cheek. Most people have some depth there. Volume loss makes it dramatic. The skin under the eye is the thinnest skin on the face, which means it cannot hide a depleted fat pad beneath it. You see the orbital rim, the underlying structure, in a way that reads as exhaustion or aging even on a face that is otherwise unchanged.
This is the area patients describe noticing first, usually before they have a name for what they are seeing. They look tired when they are not. Their under-eye concealer, which used to be optional, now feels mandatory. The hollowing is real and structural. Topical products will not reverse it. For anyone considering filler to address it, tear trough filler recovery has its own significant learning curve worth understanding before booking.
What Helps a Little
Skincare has a modest, honest role here. Collagen-supporting ingredients, retinoids, vitamin C, peptides, do contribute to skin quality and can improve the skin’s texture and firmness at the surface level. That is worth something. It does not replace volume, but better skin quality means the existing structure looks better. Think of it as improving the paint quality on a house rather than rebuilding the walls.
Adequate protein intake supports skin and tissue quality in a general way, as does staying well hydrated. These are not miracle interventions and they are not a substitute for a conversation with a dietitian if you have specific nutrition questions. The framing that matters here is maintenance, not restoration.
The single most effective prevention, if you are earlier in your weight loss, is rate. Slower weight loss gives the skin more time to adapt and gives the facial fat compartments a chance to deplete gradually rather than all at once. That said, the therapeutic effects of GLP-1 medications operate on their own timeline, and adjusting your approach to medication is a conversation that belongs exclusively with your prescribing doctor. Not a skincare article. Your doctor.
What Actually Restores Volume
If the hollowing is significant, skincare will not close the gap. The treatments that actually work are volume replacement treatments, delivered by an injector or surgeon. Here is the honest hierarchy:
Hyaluronic acid filler is the first tool most people reach for, and appropriately so. It is reversible with hyaluronidase, the results are immediate, and a skilled injector can restore the specific fat pad volume you have lost rather than just plumping generically. Cost typically runs a few hundred dollars per syringe, and the face after significant weight loss may need more than one syringe to address multiple areas. Budget accordingly and do not let a single syringe price anchor your expectations.
Biostimulators like Sculptra work differently. They do not add immediate volume. Instead, they trigger the body’s own collagen production over several months. The results take longer to appear (think three to six months for the full effect) but tend to look more gradual and naturalistic. They are also better suited for diffuse volume loss across a large area rather than a precise, localized deficit. These treatments cost more upfront and require patience. For people who lost a lot of weight, they are worth a serious conversation with an injector.
Fat grafting, where fat is harvested from another part of the body and transferred to the face, is a surgical option that some patients pursue when the volume loss is extensive. The results can be long-lasting. It also requires a surgical setting, downtime, and a surgeon rather than an injector. If you have also had body contouring procedures, your plastic surgeon may be the right person to have this conversation with.
Choosing the Right Injector for Volume Restoration
This is the part that matters most and gets skipped most often. Volume restoration after significant weight loss is not a standard filler appointment. The anatomy is different. The facial fat pads have deflated asymmetrically in most cases. The skin has lost some of its elasticity. An injector who is skilled at trend lips or Botox maintenance is not automatically the right person for this.
Patients consistently describe a pattern: they went to the most convenient or least expensive option first and ended up with filler that looked placed rather than natural, or with one area corrected while another looked worse by comparison. The consultation is where you assess whether the injector can articulate what they are seeing in your face and what they are planning to do about it, not just where and how much.
Look for someone who has specific experience treating post-weight-loss facial changes. Ask about their experience with biostimulators as well as HA filler, since significant volume loss often warrants both over time. The tear trough specifically requires a technically precise injector. Understanding what filler does to tissue over time matters for this conversation too, because the goal here is building a plan, not one treatment.
The medication decisions, including whether to continue, pause, or adjust your GLP-1 treatment, belong entirely with your prescribing doctor. Filler can coexist with ongoing treatment. It can also be planned for after you reach a stable weight, since treating volume loss while weight is still actively changing means a moving target. Your injector and your prescribing physician should ideally be in communication, or at minimum aware of each other.
FAQ
Patients wondering how tirzepatide and semaglutide compare specifically on facial and aesthetic side effects can find a detailed breakdown in the tirzepatide vs semaglutide aesthetic effects comparison.
Is ozempic face permanent?
No. The hollowing is volume loss, not structural damage, and volume can be restored. The skin changes that accompany rapid weight loss, looseness and some loss of elasticity, can be more stubborn, but they are also improvable over time with the right treatments. The key is addressing it from the right level: filler and biostimulators for the deep fat pad loss, skincare for the surface quality.
Do I need to wait until I stop losing weight before getting filler?
Not necessarily, but it is worth discussing with your injector. If you are still losing weight at a significant rate, the volume deficit will continue to shift, which means results may not be predictable. Many injectors prefer to treat at or near a stable weight. That said, some patients choose to address the most severe hollowing while still in the active weight loss phase. This is an individual decision made with your injector, not a rule either way.
What should I tell my injector about being on a GLP-1 medication?
Tell them everything. The medication, your rate of weight loss, how much you have lost, and where you are in the process. A good injector will factor this into their treatment planning, particularly around timing and how aggressive to be with volume replacement at a single appointment. Nothing about GLP-1 use makes filler unsafe, but it absolutely shapes the approach a thoughtful injector takes.
This article is for educational purposes only and is not a substitute for professional medical advice. Always follow your injector’s or surgeon’s specific aftercare instructions.