
You have your faja. You have been told to wear it consistently. What your post-op instructions may not have explained clearly is that the faja alone is not a complete compression system in the first weeks after tummy tuck or Lipo 360. Two additional tools, abdominal boards and lipo foam sheets, perform distinct mechanical functions that the garment cannot. Using the wrong one at the wrong time, or skipping either entirely, produces predictable and correctable problems. Here is the distinction that matters.
Looking for a quick answer? Jump to the FAQ below.
The short answer
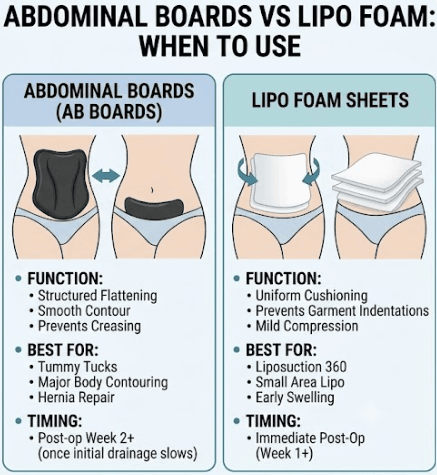
Most lipo and tummy tuck patients need both: lipo foam for the first 1-2 weeks to protect incision sites and prevent pressure marks from the faja, and an abdominal board from week 2-3 onward to smooth and flatten the treated area. They serve different purposes at different stages. Buying one and not the other is the most common mistake.
What an Abdominal Board Actually Does
An abdominal board, or ab board, is a rigid or semi-rigid compression panel, typically made of foam-padded plastic or medical-grade polypropylene. It is worn against the abdominal skin, inside the faja, positioned between the garment and your body. Its function is structural: the board provides a flat, firm, even surface against which the faja applies its compression force. Without a board, a faja applies pressure unevenly, conforming to the contours and irregularities of swollen, healing tissue. That uneven compression can create longitudinal grooves, creases, or ridges in the skin as the tissue hardens around it during early fibrosis formation. The board distributes the compression force across a smooth, uniform plane, preventing those artifacts from developing.
The second function of an ab board is abdominal projection management. After tummy tuck procedures, the abdominal wall has been tightened surgically. An ab board applies consistent, flat pressure that encourages the tissue to heal in a flat, projected position rather than allowing the initial post-op puffiness to become the new baseline. Patients who have also undergone hernia repair alongside their tummy tuck are frequently prescribed boards as part of their abdominal wall support protocol.
Ab boards are best suited for tummy tucks, major body contouring including Lipo 360 with significant abdominal work, and any procedure where the surgeon has specifically noted concern about abdominal projection or scar formation patterns. They are not a universal tool. Patients who had only minor, localized liposuction to flanks or outer thighs may have no need for a board at all.
Recommended: Ab Board
An ab board only works if it spans from under the bust down to the lower abdomen, covering the full treated zone. For Lipo 360, this front and back board set covers both sides of the treatment area without needing a second purchase.
What Lipo Foam Sheets Do Differently
Lipo foam is a soft, open-cell foam sheeting product, typically one quarter to one half inch thick, worn between the skin and the faja — for step-by-step guidance, see the full guide on lipo foam placement. It is fundamentally different from an ab board in both material and mechanical purpose. Where a board is rigid and distributes compression over a single flat plane, lipo foam is pliable and functions as a cushioning interface that standardizes the contact pressure between the garment and all surface irregularities simultaneously.
Immediately after liposuction, the tissue surface is uneven. Edema pools unevenly. Cannula tunnels create micro-depressions. The faja, pressing against this landscape, applies high pressure at tissue peaks and near-zero pressure in the valleys. Lipo foam fills those valleys. It conforms to the irregular surface and ensures the faja pressure is transmitted uniformly across the entire contact area. This prevents the garment from imprinting its seams, edges, or boning into the softened, trauma-responsive tissue as it begins to harden.
Lipo foam is also appropriate for areas where an ab board would be impractical: the flanks, back, and lateral thigh. For Lipo 360 patients, foam sheeting is typically prescribed for the full circumferential treated area, providing consistent mild compression across all zones without the rigidity of a board. For smaller, localized lipo procedures, foam alone is usually sufficient and is the standard recommendation in the first week.
Recommended: Lipo Foam
Foam sheets sit between your skin and the faja to spread compression evenly across the treated area instead of letting the garment press unevenly on healing tissue. Because sheets compress and wear out over weeks of daily wear, this medical-grade foam multi-pack keeps fresh sheets on hand for the full recovery stretch.
Abdominal board vs. lipo foam: at a glance
| Feature | Abdominal Board | Lipo Foam |
|---|---|---|
| Primary purpose | Flattening and smoothing | Cushioning and pressure distribution |
| Material | Firm plastic or foam board | Soft open-cell foam |
| When to start | Week 2-3 post-op | Day 1-2 post-op |
| Worn | Under the faja against the skin | Between skin and faja |
| Procedures | Lipo, tummy tuck, lipo 360 | Lipo, BBL, tummy tuck |
| Can they be used together | Yes — board under foam under faja | Yes — see above |
| Average cost | $15-40 | $10-25 for a pack |
The Critical Timing Gap Between the Two
This is where most patients go wrong. Lipo foam is an immediate post-operative tool. It goes on within the first week of surgery, often the first day, worn inside the faja from the moment you leave the surgical center. Abdominal boards are not. Placing a rigid board against fresh, draining, actively inflamed tissue is contraindicated in the first weeks of recovery. The firmness of the board can impede drainage, compress swollen tissue against intact surgical sutures, and create pressure differentials that concentrate force exactly where you do not want it.
The standard transition point for introducing an ab board is post-operative week two, and only once your surgeon confirms that initial drainage has slowed significantly. The practical indicator is usually the removal or cessation of drain output, if drains were placed. Some surgeons prefer to introduce boards at week three or even week four for patients with more extensive tissue work. The decision is always surgeon-directed and should not be self-initiated based on online advice or the timeline a garment supplier suggests.
Once you transition to an ab board, lipo foam does not disappear from your protocol. For many patients, foam continues to be worn behind the board, against the skin, while the board sits between the foam and the faja. This layered arrangement provides both the cushioning interface of the foam and the structural flattening of the board simultaneously. For the complete garment transition framework, including when to move from Stage 1 to Stage 2 compression, see our guide on Stage 1 vs Stage 2 faja: when to switch and sizing guide.
The Layering Guide: How They Stack Under Your Faja
Correct layering order is not obvious to most patients, and reversing it makes both tools less effective. The correct sequence, from skin outward, works as follows.
Layer 1, skin contact: If you are in weeks one and two, lipo foam sits directly against your skin. It should be cut or folded to cover the full treated area without creating hard edges that could imprint at the seam lines. The foam side with the larger open cells typically faces the skin for maximum airflow. If your foam came with a smooth side and a textured side, ask your surgical team which orientation they recommend. Their protocol may specify one direction for abdominal work and the opposite for flanks.
Layer 2, the ab board (from week two onward): The ab board sits on top of the lipo foam, not directly on the skin. Its smooth face points inward, against the foam. Position it centered over the abdomen, below the navel line for most tummy tuck patients, though your surgeon may specify higher or lower placement depending on where tightening was performed. The board should not extend past the edges of your faja’s coverage area, as overhanging rigid material creates a pressure edge effect that can bruise soft tissue laterally.
Layer 3, the faja: The compression garment goes over everything. It holds both the foam and the board in position and provides the inward compression force. If your faja is a Stage 1 garment with front hook-and-eye closures, fasten from the bottom upward to prevent downward displacement of the foam and board as you compress. If you are already in a Stage 2 pull-on garment, ensure the foam and board are fully positioned before pulling the garment up over them.
Common Mistakes and How to Avoid Them
Using an ab board too early. The most common error and the one with the most potential for harm. A rigid board applied before drainage has slowed can create a pressure compartment beneath the skin that prevents fluid from reaching its exit pathways. If you were given a board by a non-surgical provider or purchased one based on a social media recommendation, do not introduce it before your surgeon explicitly approves the timing.
Skipping lipo foam entirely. Some patients receive fajas and boards without foam, either because their surgical team did not emphasize it or because they ordered garments from a generic supplier. This gap in the protocol means the faja is pressing directly against uneven tissue with no cushioning interface. The result is often visible garment seam imprints in the hardening skin, asymmetric compression artifacts, and increased discomfort at boning locations.
Using foam that is too thick or too thin. Standard lipo foam thickness for abdominal applications is one quarter to three eighths of an inch. Foam thicker than half an inch begins to reduce the net inward compression force of the faja by acting as too much of a buffer. Foam thinner than an eighth of an inch does not provide sufficient cushioning to equalize pressure.
Wearing the board without the foam beneath it. A rigid board in direct skin contact creates hard-edge pressure points at the board’s perimeter. These edges can dig into healing tissue over hours of wear and create localized bruising or compression marks that temporarily worsen in appearance before improving.
Stopping both tools too soon. Tissue is not fully stable until month three to month four post-operatively. Patients who discontinue compression aids at four to six weeks because swelling appears resolved often find that residual tissue pliability allows mild asymmetries to develop as final fibrosis sets in. Continue wearing foam and board for the full duration your surgeon prescribes, even when the mirror suggests you are done. Pairing consistent compression use with a structured lymphatic massage schedule gives your tissue the best chance of resolving smoothly.
This is normal
- Pressure marks or indentations from the board that fade within an hour of removal
- Board shifting position during the day — reposition and continue
- Mild skin irritation in the first few days as skin adjusts
- Foam compressing and flattening over time — replace when it no longer provides cushion
Call your surgeon if
- Skin breakdown or open areas where the board or foam contacts the skin
- Numbness that does not resolve after removing the garments for an hour
- Swelling that is suddenly worse after starting board use
- Any wound complications at incision sites near where the board sits
This article is for educational purposes only and is not a substitute for professional medical advice. Always follow your injector’s or surgeon’s specific aftercare instructions.